by Janet Munu
Problem/Significance
The United States is deemed a wealthy country, but the problem of food insecurity is prevalent. Feeding America, a hunger-relief organization in the United States, reported that 34 million people in the US, including 9 million children, face food insecurity (Feeding America, 2023). The growing need for food insecurity needs attention.
The United States Department of Agriculture's (USDA) definition of food insecurity "is the limited or uncertain availability of nutritionally adequate and safe foods or limited or uncertain ability to acquire acceptable foods in socially acceptable ways." USDA categorizes food security and insecurity into the following categories (The United States Department of Agriculture, 2023).
-
High food security: “no reported indications of food-access problems or limitations”.
-
Marginal food security: “one or two reported indications—typically of anxiety over food sufficiency or shortage of food in the house. Little or no indication of changes in diets or food intake”.
-
Low food security: “Reports of reduced quality, variety, or desirability of diet. Little or no indication of reduced food intake.”
Very low food security: “Reports of multiple indications of disrupted eating patterns and reduced food intake.”
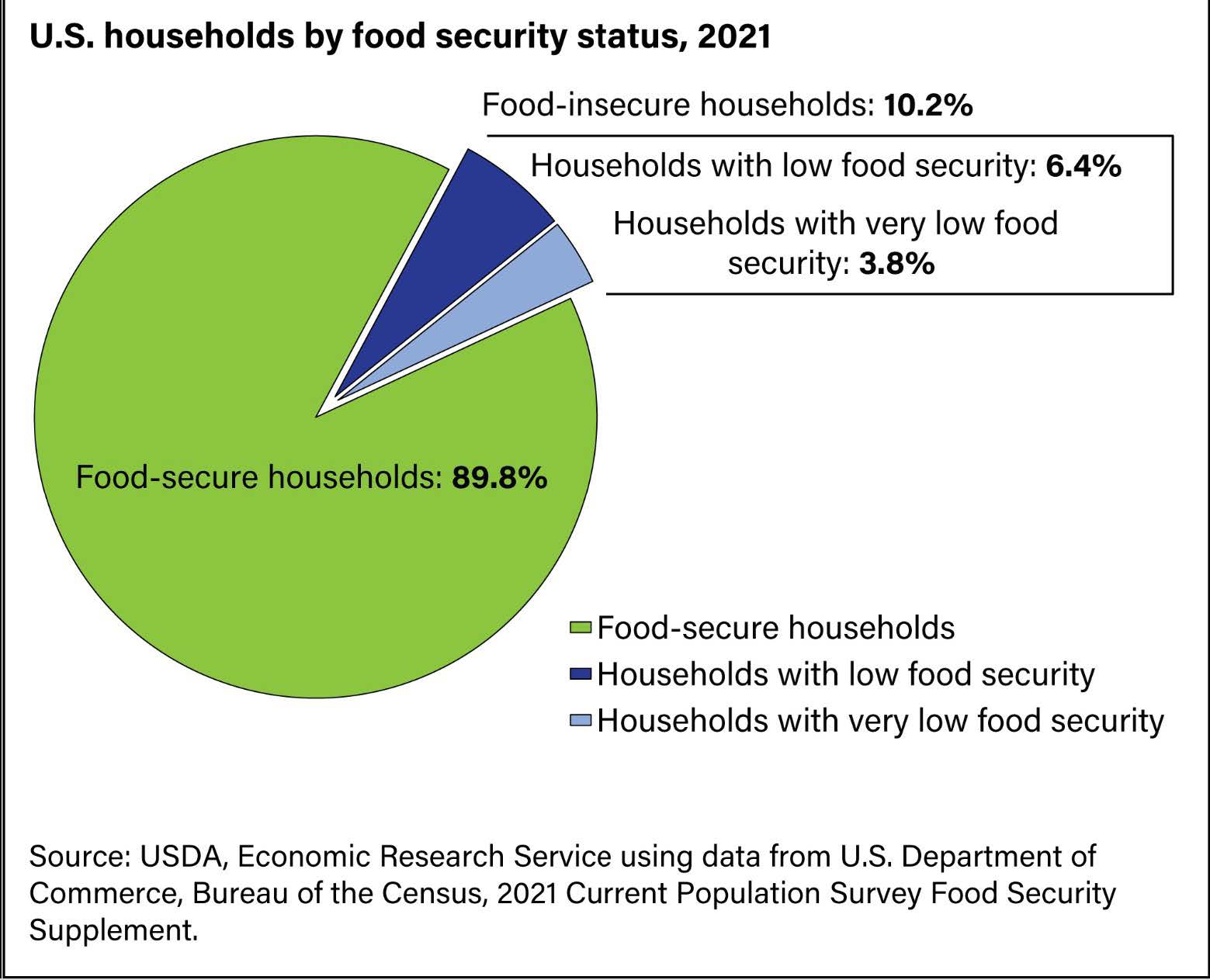
The image below shows the prevalence of food insecurity in the U.S. household Food Insecurity
Statistics.
Food Insecurity and Cancer Care
Food insecurity is a growing concern among cancer patients, impacting their nutritional status and overall health. A study by Ganey et al. (2021) referenced that medically underserved cancer patients are more likely to be food insecure than the general population. In addition, based on the study of a cohort of underserved cancer patients in New York City, 56% of patients were food insecure; 38% had very low food security.
Cancer patients experience physical and emotional turmoil during their treatment and care. According to Gany et al. (2014), they represent a vulnerable population because of the disease process and the intensity of treatment protocols. During this phase, cancer patients require access to healthy food and adequate nutrition to maintain their energy levels, optimize immunity, and respond to treatment. Food insecurity is also associated with non-adherence to treatment protocols.
Several studies on food insecurity's impact on cancer care show evidence that it can contribute to adverse health consequences among cancer patients. They are prone to poor functional, social, and emotional well-being. Limited access to nutritious foods can lead to malnutrition, weight loss, and fatigue and impact their quality of life. These can undermine cancer treatment and increase the risk of complications. Individuals experiencing food insecurity tend not to seek medical care, and noncompliant with the treatment regimen, and miss appointments (Simmons, 2006). Furthermore, Mendoza (2022), speculates that the severity of food insecurity may lead to depression, and anxiety, impairing the ability to access preventive healthcare services such as screening for cancer.
Cause of Food Insecurity
Factors contributing to food insecurity among cancer patients include the high cost of cancer treatment, reduced income due to work disruption, and transportation barriers to healthy food. Food insecurity is also associated with non-adherence to treatment protocols Bengle (2010). Furthermore, cancer patients experience psychological stress, anxiety, or depression, which may exacerbate food insecurity by reducing their motivation to eat.
Addressing Food Insecurity
Addressing food insecurity among cancer patients is critical for improving their treatment outcomes and overall well-being. Below are suggested measures to address food insecurity for cancer patients.
-
Enable patients with transportation to the local grocery stores and access to health care.
-
Provide direct food assistance such as Meals on Wheels.
-
Healthcare organizations are encouraged to screen patients for food insecurity (Feeding America, Simmons (2006). Screening cancer patients for food insecurity takes limited time but has the potential to have significant improvement in patient outcomes ASCO (2022)
Refer patients to food assistance programs, connect patients to Supplemental Nutrition Assistance Program (SNAP), community food banks, senior meal programs, and up food set distribution to address the immediate need.

Healthcare Addressing Food Insecurity

Considerations for Future Work:
-
Raise awareness and advocate for policy changes.
-
To positively impact patients' health and improve clinical outcomes, it is essential to extend care beyond the walls of the healthcare system and provide longitudinal care for patients with food insecurity.
-
Gany (2021) suggests that cancer clinics set up a system with patient navigators, nutritionists, education and outreach coordinators, and social workers, case managers to provide comprehensive and timely assistance.
-
Further research is needed to develop or use an existing framework to address food security based on the theories of Poverty.
Conclusion
In addition to providing cancer treatment, addressing food insecurity is crucial in cancer care. It is imperative to incorporate policy changes, collaborative research, implementing processes, and monitoring patients to ensure that cancer patients receive proper nutrition during and after treatment. Addressing the issue is essential for improving patient outcomes, overall health, and quality of life.
References
-
Bengle R, Sinnett S, Johnson T, Johnson MA, Brown A, Lee JS. Food insecurity is associated with cost-related medication non-adherence in community-dwelling, low- income older adults in Georgia. J Nutr Elder. 2010 Apr;29(2):170-91. doi: 10.1080/01639361003772400. PMID: 20473811.
-
Feeding America. (2023). What is Food Insecurity. Retrieved 2023 March 15 from https:// www.feedingamerica.org/hunger-in-america/food-insecurity
-
Gany F, Lee T, Ramirez J, Massie D, Moran A, Crist M, McNish T, Winkel G, Leng JC. Do our patients have enough to eat?: Examining the Association of Food Insecurity. J Health Care Poor Underserved. 2014 Aug;25(3):1153-68. doi: 10.1353/hpu.2014.0145. PMID: 25130231; PMCID: PMC4849892.
-
Gany F, Melnic I, Ramirez J, Wu M, Li Y, Paolantonio L, Roberts-Eversley N, Blinder V, Leng J. The association between housing and food insecurity among medically underserved cancer patients. Support Care Cancer. 2021 Dec;29(12):7765-7774. doi: 10.1007/s00520-021-06254-1. Epub 2021 Jun 24. PMID: 34169329; PMCID: PMC8225310.
-
Mendoza JA, Miller CA, Martin KJ, Resnicow K, Iachan R, Faseru B, McDaniels- Davidson C, Deng Y, Martinez ME, Demark-Wahnefried W, Leader AE, Lazovich D, Jensen JD, Briant KJ, Fuemmeler BF. Examining the Association of Food Insecurity and Being Up-to-Date for Breast and Colorectal Cancer Screenings. Cancer Epidemiol Biomarkers Prev. 2022 May 4;31(5):1017-1025. doi: 10.1158/1055-9965.EPI-21-1116. PMID: 35247884; PMCID: PMC9135358.
-
Simmons LA, Modesitt SC, Brody AC, Leggin AB. Food insecurity among cancer patients in kentucky: a pilot study. J Oncol Pract. 2006 Nov;2(6):274-9. doi: 10.1200/JOP.2006.2.6.274. PMID: 20859354; PMCID: PMC2793655.
-
U.S. Department of Agriculture, Economic Research Service. (n.d.). Key statistics & graphics. Retrieved April 29, 2023 from https://www.ers.usda.gov/topics/food-nutrition- assistance/food-security-in-the-us/key-statistics-graphics.aspx
-
https://hungerandhealth.feedingamerica.org/explore-our-work/community-health-care- partnerships/addressing-food-insecurity-in-health-care-settings/











